User login
Language
Anonymous's groups in this site
User is not a member of any group.
Your groups across all your sites
User is not a member of any group.
Recent Content
Who's online
There are currently 0 users online.
You are here
Impacts of flood on health: epidemiologic evidence from Hanoi, Vietnam
Primary tabs
Impacts of flood on health: epidemiologic evidence from Hanoi, Vietnam
Thu, 2011-11-17 04:23 — adminBackground: Vietnam is one of the most disaster-prone countries in the world. The country suffers from many kinds of natural disasters, of which the most common and serious one is flooding. Long and heavy rainfall during the last days of October and the first week of November 2008 resulted in a devastating flood unseen for over three decades in the capital city of Hanoi. It caused a substantial health impact on residents in and around the city and compromised the capacity of local health services.
Objective: The aim of this study is to ascertain the vulnerability and health impacts of the devastating flood in Hanoi by identifying the differences in mortality, injuries, and morbidity patterns (dengue, pink eye, dermatitis, psychological problems, and hypertension) between flood affected and non-affected households.
Design: A cross-sectional study was carried out involving 871 households in four selected communes (two heavily flood affected and two comparatively less affected) from two severely flooded districts of Hanoi. Participants were interviewed and information collected on the social, economic, and health impacts of the devastation within 1 month after the flood.
Results: The self-reported number of deaths and injuries reported in this study within 1 month after the heavy rainfall were a bit higher in severely affected communes as compared to that of the less affected communes of our study. The findings showed higher incidences of dengue fever, pink eye, dermatitis, and psychological problems in communes severely affected by flood as compared to that of the controlled communes.
Conclusions: For people in flood prone areas (at risk for flooding), flood prevention and mitigation strategies need to be seriously thought through and acted upon, as these people are exposed to greater health problems such as psychological issues and communicable diseases such as pink eye or dermatitis.
1Department of Epidemiology, Hanoi School of Public Health, Hanoi, Vietnam; 2Centre for Research
on the Epidemiology of Disasters, Universite´ Catholique de Louvain, Louvain-la-Neuve, Belgium
Authors: Tran Huu Bich1, La Ngoc Quang1, Le Thi Thanh Ha1*, Tran Thi Duc Hanh1 and Debarati Guha-Sapir2
Global Health Action 2011. # 2011 Tran Huu Bich et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License (http://creativecommons.org/licenses/by-nc/3.0/), permitting all non-commercial use, distribution, and reproductionin any medium, provided the original work is properly cited.
Citation: Global Health Action 2011, 4: 6356 - DOI: 10.3402/gha.v4i0.6356
Received: 12 February 2011; Revised: 11 July 2011; Accepted: 29 July 2011; Published: 23 August 2011
Flooding accounts for about 40% of all natural disasters worldwide and causes about half of all deaths (1, 2). The greatest potential flood hazard is in Asia. Every year for the past two decades more than 400 million people on average have been directly exposed to floods. Between 1987 and 1997, 44% of all flood disasters worldwide affected Asia, claiming 228,000 lives (roughly 93% of all flood-related deaths worldwide) (3). Vietnam is one of the most disaster-prone countries in the world. The country suffers from many kinds of natural disasters, of which the most common and serious one is a flood (4). In 2007, it was estimated that 400 people died from floods and the economic loss was estimated around 11.5 billion VND (about US$650 million) (5). Threat of climate change, altered patterns of precipitation, and rise in sea level are believed to increase the frequency and intensity of floods in many regions of the world (6, 7).
The health consequences of floods may be described in relation to time (e.g. as intermediate, mid-term, and long-term). The recognised immediate health effects of flooding include drowning, injury, acute asthma, skin rashes and clusters, outbreaks of gastroenteritis, and respiratory infections (1, 810). The mid-term effects of flooding are infected wounds, complications of injury, poisoning, poor mental health, communicable diseases, and starvation (11). In the long-term chronic disease, disability, poor mental health, and poverty-related diseases including malnutrition are the potential legacy (2, 11). The long-term effects of flooding on health may perhaps be even more important than other illnesses or injuries because the psychological problems may continue for long after the water has receded (2). Floods with long duration cause serious health problems for local people, particularly of the elderly and disabled family members living in poor conditions with limited food stocks, unhygienic water sources, and poor sanitation. Epidemic diseases such as dengue fever, diarrhea, among many others also appeared after floods (12). However, as Few et al. note in their recent comprehensive review, there has been only limited systematic research on the health outcomes of flooding (12).
Long and heavy rainfall during the last days of October and the first week of November 2008 resulted in the most devastating flood since 1973 in the capital city of Hanoi. Heavy rains in the inner part of Hanoi on October 31st caused 90 points inundated locally with an average depth of 0.3 m0.8 m. Particularly, there were points inundated with the depth up to 1.2 m in places like Thai Ha, Truong Chinh, and Giap Bat roads; and from 1.0 to 2.5 m in places like Tan Mai and the Dinh Cong areas (5). According to a primary evaluation of the 10 days of heavy rainfall and flooding (from October 31 to November 9, 2008), 22 people died and 3 were injured. Even about a month after the heavy rainfall in Hanoi, some areas were still deeply inundated.The above mentioned damages of the flood in Hanoi in terms of the deaths and injuries were just very preliminary. It is expected that the long-term impacts on the economic, social, environmental, and health aspects of people living in Hanoi would be significant (5).
In order to ascertain the flood vulnerability, health risks, and social and economic impacts of the devastating flood in Hanoi, a cross-sectional study was conducted through a household survey. This paper used data collected from the MICRODIS household survey early 2009 in Hanoi, Vietnam, which is part of a wider research project involving 15 other countries from Europe and Asia. The MICRODIS is an Integrated Project funded under the EU Sixth Framework Programme Thematic Priority 6.3 Global Change and Ecosystems (Contract number GOCE-CT-2007-036877).
The aim of this paper is to identify the differences in mortality, injuries, and morbidity patterns (dengue, pink eye, dermatitis, psychological problems, and hypertension) between flood affected and non-affected households in Hanoi after the historic flood in 2008. The ultimate aim of this paper is to provide information for designing appropriate early response to flood and preventive strategies for flood prone areas.
METHODOLOGY
Data Source
The data in this paper were obtained from the MICRODIS project’s household survey 2009. The survey was conducted in two districts: Hoang Mai (urban district) Chuong My (rural district) in Hanoi capital city of Vietnam. In each district, a severely flooded commune and a less affected commune (control commune) were selected with reference to the district’s people committee; households were then randomly selected from the lists of households in each selected commune. The head of the household or his/her counterpart was the key respondent.
There were 871 people interviewed at the household level by trained fourth year students of the Hanoi School of Public Health. Data quality was controlled by the field supervisors as well as by the investigators of this survey. The survey questionnaire was adapted from the MICRODIS integrated questionnaire and included three main themes: health, economic, and social. Each theme was adapted from internationally validated questionnaires that were later confirmed by the members of each working group of the MICRODIS project.
Measurement
Information on five health conditions were collected through self-reported method (two non-communicable: psychological problem and hypertension and three communicable diseases: dengue fever, pink eye, and dermatitis) as follows:
Key respondent was asked ‘Have any of your family members ever had psychological problems, e.g. stress, nervous, anxious, sleeplessness, etc.’ The answering options were yes/no. If the answer is yes, then each diseased person in the household was asked through the key respondent whether the psychological problem occurred before the heavy rains or after and, if it occurred before the heavy rains, then whether the condition got worse after the heavy rains/flood.A similar question was asked for hypertension with a special emphasis on diagnosis of hypertension by a health officer. For communicable diseases, the respondent was first asked ‘Have any of your family members ever been diagnosed by a health officer as having the disease.’ The answering options were yes/no. Then each diseased person in the household was asked through the key respondent whether the disease occurred within 1 month after the heavy rains/flood.
Mortality and injuries of family members of study subjects were also measured by the self-reported method within 1 month since the heavy rains started. Information on socio-demographic status of study subjects included educational level, gender, religion, age, marital status, and income per person per month.
Data Analysis
Epidata 3.0 was used for data entry. SPSS software version 17 was used to perform both descriptive and analytical statistics. A conventional significance level of pB0.05 was used.
Ethical Considerations
Before collecting data in the field, the protocol was submitted to the internal review board (IRB) at the Hanoi School of Public Health. The study was presented and discussed among provincial authorities for their approval. Approval was also received from key informants before carrying out the interview.
RESULTS
Characteristics of Study Population
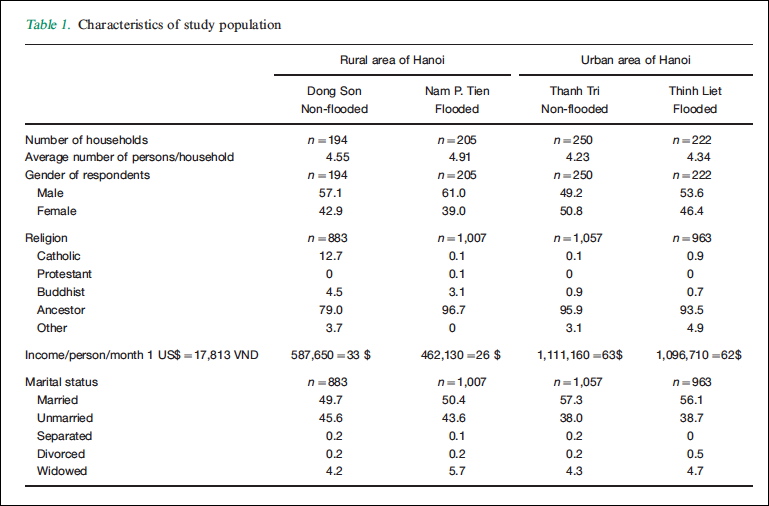
A total of 781 respondents participated in the MICRODIS household survey 2009. The description of the final sample is presented in Table 1. Among the respondents, the proportion of males was higher than that of the females, except for Thanh Tri commune where the proportion of females was a little bit higher (50.8% vs. 49.2%). The average number of persons per household was highest in Nam P. Tien (4.91), a severely flooded commune in rural area of Hanoi, and lowest in Thanh Tri, a less affected commune in urban area of Hanoi. Almost all of the people in our sample population said that their religion is to pray to ancestors with about 12% of respondents in the Dong Son commune being Catholics. Buddhists formed about 1% of the respondents from Thanh Tri and Thinh Liet urban communes of Hanoi and also those from Dong Son and Nam P. Tien 4.5 and 3.1%, respectively, were Buddhists.
The income per person per month of urban communes in Hanoi is almost double that of rural communes of Hanoi. Within rural areas, a significant difference in income between the severely affected commune and the less affected commune (33$ vs 26$ per person per month) was observed. With regards to marital status, about half of our studied population were married, about 40% were unmarried, and about 5% widowed.
Experience With the Heavy Rainfall/Flood
Results from Table 2 shows that almost all people in our sample were present at the time of the heavy rainfalls/ flood (greater than 97% in all four communes). About half of the people in Nam P. Tien had to migrate due to flooding and in Thinh Liet the number was about 20%. The proportion of people in the two less affected communes who had to migrate due to flooding was very low (1.6% in Dong Son and 2.3% in Thanh Tri). The majority of people who migrated due to flooding stayed in their relative’s or friend’s house within their commune. In addition, people living in communes that were severely affected by flood reported that they stayed in temporary shelters provided by the government such as in schools, community houses, etc.
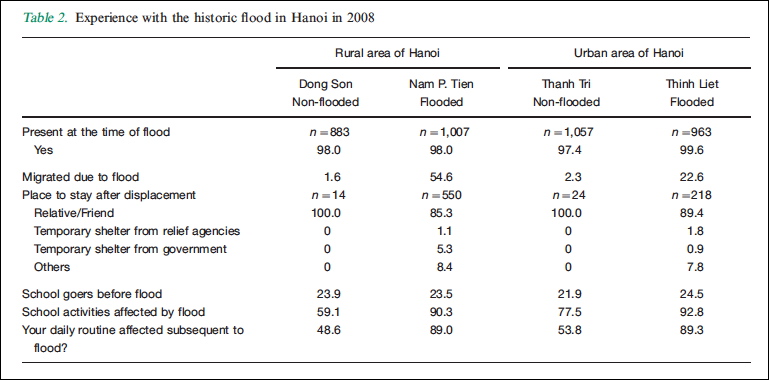
About a fourth of the members of our study sample were going to school before the heavy rains that led to the historic flood in Hanoi. Ninety percent of the school goers in two severely affected communes said that school activities were affected (flooded and closed subsequently) by the flood. Amongst the less affected communes in Dong Son and Thanh Tri, about 66% of schools and 75% of school goers, respectively, said that school activities were affected by the rainfalls. Ninety percent of the respondents from the two severely affected communes and 50% of those from the less affected communes mentioned that daily routine work was affected subsequent to the flood.
Access To and Use of Usual Health Care Service/ Medication
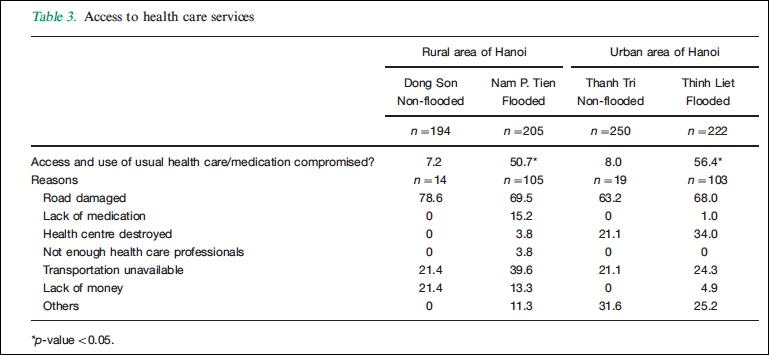
Almost half of the respondents in both severely flooded communes said that the access to and use of their usual health care/medication were compromised during 1 month since the heavy rains and/or flooding (Table 3). These proportions were much lower in two communes that were not severely flooded (7 or 8%). With regards to the question about the reasons why the access and usual health care/medication were compromised by the heavy rainfalls/flood, respondents could give multiple reasons. Among those who said that their access to usual health care or medication was compromised, about two-thirds mentioned that one of the reasons was damaged roads and one-third mentioned unavailability of transportation. One-fifth of the respondents in Thanh Tri and one-third of the respondents in Thinh Liet said that the health centre was destroyed. About 15% of respondents in the Nam P. Tien commune said that it was due to lack of medication or lack of money.
Mortality
In our sample during 1 month after the heavy rain in Hanoi that led to flooding, seven deaths were reported, three from Nam P. Tien, two from Thinh Liet, and one death occurred in each less affected commune. Of the two deaths in Thinh Liet, one occurred during the day of the flood and one occurred within the week following the flood. One death in Dong Son, one death in Thanh Tri and two deaths in Nam P. Tien occured during the month following the flood. Two out of seven deaths were reported to be cancer, three others were due to stroke, and the rest (two) were from other causes; four of the seven deaths were reported to be confirmed by a physician or nurse. All seven deaths took place in the individual’s respective homes.
Injuries
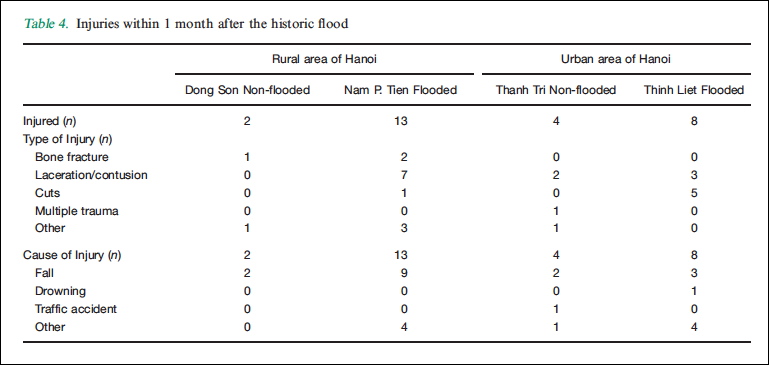
Twenty-seven injuries were reported 1 month after the heavy rainfall/flooding. Types of injuries are reported in Table 4. Three persons suffered bone fracture, one from Dong Son and two from Nam P. Tien. Twelve people suffered lacerations and/or contusions. Seven of these people were from Nam P. Tien, two of them from Thanh Tri, and three lived in Thinh Liet. Two-thirds of the injuries were reported due to falls. Thirteen injuries occurring in Nam P. Tien, nine were due to falls, one person was injured in Thinh Liet due to drowning, and one in Thanh Tri was injured in a traffic accident. Falls and drowning seem to be the attributable injuries to flooding.
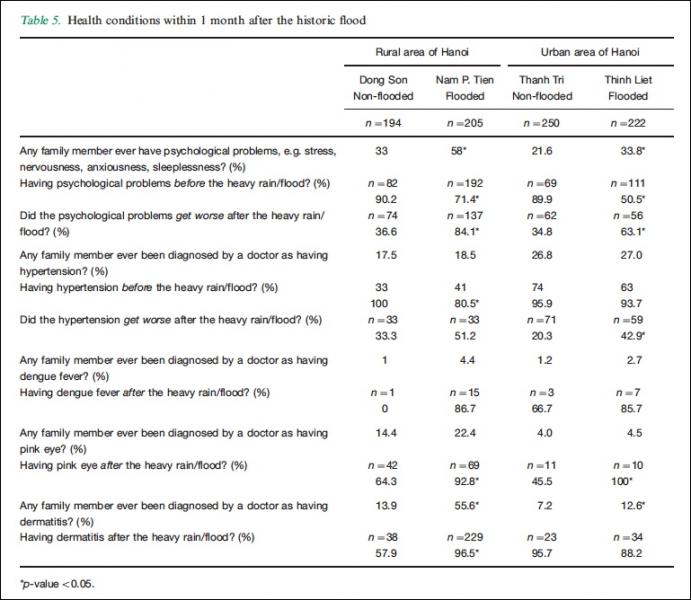
Health Conditions
Health conditions of people in this survey were measured through a self-reported method. The key respondent was in charge of providing information for other family members. The results are presented in Table 5. There were significant differences between the respondents from severely affected commune and those from the less affected communes in terms of the family members suffering from psychological problems. In less affected communes about 90% of people who ever had suffered from psychological problems were reported to have had experienced it before the heavy rains and the flooding, while these proportions in the two severely affected communes of Nam P. Tien and Thinh Liet were 72 and 50%, respectively. Only about one-third of those suffering in less affected communes said that their psychological problems got worse during and after the flood, while the percentage of people in severely affected communes (Nam P. Tien and Thinh Liet) with worsening psychological problem during and after the flood were 84.1 and 63.1%, respectively. These differences are statistically significant.
There is no significant difference in the number ofrespondents reporting that his/her family members hadever been diagnosed with developing hypertensionbetween the heavily flood affected commune and less affected commune in the rural or urban district of Hanoi. Although almost all reported cases of hypertension occurred before the heavy rain/flood, the percentage of people reporting that it got worse after the flood was significantly higher in the severely affected commune than that of the less affected commune in the urban district (20.3% in Thanh Tri and 42.9% in Thinh Liet).
Twenty-five people of the sample who reported having ever been diagnosed by a doctor for dengue fever, 15 of them were found in Nam P. Tien, and 7 in Thinh Liet, 3 in Thanh Tri, and only one case occurred in Dong Son. The majority of all cases in the affected communes reported that they were diagnosed with dengue fever after the flood (86.7% in Nam P. Tien and 85.7% in Thinh Liet). Two out of three cases in Thanh Tri occurred after the flood. There were no statistically significant differences in the proportion of dengue cases in flood affected and less affected communes.
With regards to pink eye, the number of respondents mentioned that his/her family member ever having pink eye was quite low, about 4% in both the affected and less affected commune in urban area of Hanoi, these proportions were a bit higher in rural areas of Hanoi (14.4% in Dong Son and 22.4% in Nam P. Tien). In both flood affected communes, almost all people who ever had suffered from pink eye were reported to have got pink eye after the flood (92.8% in Nam P. Tien and 100% in Thinh Liet). These proportions in two less affected communes were significantly lower with 64.3% in Dong Son and 45.5% in Thanh Tri.
With regards to dermatitis, about 56% of respondents in Nam P. Tien reported that a person from the family had ever been diagnosed by a doctor with dermatitis. This number was significantly lower in its control commune, Dong Son (13.9%). The percentage of people in the urban district who had dermatitis was low in Thinh Liet (12.6%) with a significantly lower percentage in its control commune Thanh Tri (7.2%). And almost all dermatitis cases reported were diagnosed by the health staff after the flood.
Discussion
Chuong My, a rural district located in the extended area of Hanoi in August 2008 and Hoang Mai, an urban district located in the old area of Hanoi were selected to be the Hanoi’s flood study sites because these were the most severely inundated districts in Hanoi city after the heavy rainfalls on the last days of October and first days of November 2008. The study population (Table 1) showed that there are some differences in demographic characteristics of subjects between the communes in the rural and urban district of Hanoi such as income per person per month, average number of persons per household, and marital status. These variations reflect the difference between urban and rural districts and it was the reason why we separated our data analysis. Within each district there seems to be similar demographic characteristics between severely flooded commune and its control, which is a good indicator of comparability at baseline between the two types of sites and for our later comparisons of flood impacts on health access and health conditions.
Our study sample covers people who were present in Hanoi and witnessed heavy rainfalls/flooding that occurred in the whole area of Hanoi capital city. The number of people in Nam P. Tien who were displaced was quite high because the commune was seriously flooded. It is located in the flood dividing area of Hanoi city. One cultural characteristic of Vietnamese people is that they often have close relationships with relatives and friends and tend to live near each other. For that reason, the first option for those who had to evacuate their home was to move to a relative or friend’s house nearby, followed by other options such as moving to the community house, schools, and so on. When planning preventive and alleviation strategies during the rainy season, such relocation options should be taken into consideration.
Flooding has compromised access to crucial health services in many countries where infrastructure is poor and the population at risk has limited economic resources (13, 14). Our study showed similar results. In this study we found that the usual health care services and medication for people were not available for 50% of residents in both urban and rural flood affected communes. This was mainly due to roads heavily damaged by rain and unavailable transportation facilities. An epidemiologic review revealed that in developing countries accurate information on the mortality impact of flood events is particularly limited (12). In this study, 7 deaths were reported in 781 households (3,910 people) within 1 month of the flood though the causes of death (cancer, stroke, and others) were not necessarily a consequence of the flood. A similar result was found in the study of Kunii et al. who conducted a cross-sectional survey after the 1998 floods in Bangladesh and of 3,109 people from flood-affected households, seven (0.23%) died during (but not necessarily a consequence of) the flood two from diarrhea, two from suspected heart attacks, and three from undetermined/unrecorded causes (15).
When it comes to injuries, the result showed that falls and drowning were the major cause of injuries occurring within 1 month of the flood. Flood prevention and mitigation strategies should warn people in the flood prone area about these potential dangers.
With regards to health conditions, although this study is just a snapshot of the heath situation of residents in four studied communes within 1 month after the heavy rains/flooding in Hanoi, the findings revealed higher proportions of pink eye, dermatitis, and psychological problems in severely affected communes as compared to that of the controlled communes. These findings help for additional evidence to the current weak base when assessing the health impacts of flooding (11, 12, 16). Few et al. note in their recent comprehensive review there has been only limited systematic research on the health outcomes of flooding (12). Hajat et al. also highlight the lack of good quantitative data available on the health effects of flooding, resulting in the uncertainty about the full range of potential health impacts (17).
A major limitation of our study was the necessity to collect data on health and mortality by the self-reported method, but as this study was just part of a larger project in which data was collected from 15 other countries in Asia and Europe within limited time, adoption of any other alternative was not feasible. In addition, with the nature of a cross-sectional study, causal relationship cannot be proven but results from this study suggested that people living in flood prone areas do face greater health problems than people in less affected areas. Although we cannot claim that our sample is representative of Vietnamese people living in flood prone areas, this study is one of the very first of its kind that has examined the health impacts of floods in Vietnam.
In conclusion, results from this study suggest that flood prevention and mitigation strategies need to be put in place in flood prone areas because these people are exposed to greater health problems such as psychological issues, and communicable diseases such as pink eye or dermatitis. It is important that those who provide medical care need to be aware of the increased medical and mental health needs of the people who have experienced floods. Suffering with psychological issues may continue long after the water has receded. In the future, if flood events become more common and severe, improving the services available to people at the time of a flood event and during the recovery period may be important to improve their mental health and to reduce the burden on medical services. Our experience shows that further research is needed for better health measures and stronger epidemiological designs like cohort studies to improve understanding of the risks of flooding and the long-term consequences on people’s health. Similar studies are also required about the mechanisms by which such consequences can best be prevented or alleviated by more rigorous epidemiological studies.
Acknowledgements
This study was supported by a grant from the MICRODIS project. MICRODIS is an Integrated Project funded under the EU Sixth Framework Programme Thematic Priority 6.3 Global Change and Ecosystems (Contract number GOCE-CT-2007-036877). The authors would like to acknowledge the EU for financing this work, Professor Guha-Sapir as a coordinator of the MICRODIS project and other members of the health group and social group of the MICRODIS project for contributing to the development of the questionnaire of the Hanoi MICRODIS survey.
Conflict of Interest and Funding
The authors report no conflicts of interest. The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
References
1. Noji EK. Natural disasters. Crit Care Clin 1991; 14: 271-92.
2. Ohl CA, Tapsel S. Flooding and human health: the dangers
posed are not always obvious. BMJ 2000; 321: 1167-8.
3. United Nations University, 13 June 2004, via EurekAlert!;
NASA’s Earth Observatory. Available at: http://radio-weblogs.
com/0105910/2004/06/15.html
4. Vietnam News Agency 23/05/2008 11:17 AM.
5. Report of Hanoi capital city’s People Committee on heavy rain
situation, inundation, damages, and measures to overcome the
situation dated 03 November 2008.
6. Intergovernmental Panel on Climate Change. Climate
change 2001: impacts, adaptation, and vulnerability. Cambridge:
Cambridge University Press; 2001.
7. World Health Organization. Climate change and human health:
impact and adaptation; 2000. Available from: http://whqlibdoc.
who.int/hq/2000/WHO_SDE_OEH_00.4.pdf
8. Baxter PJ, Moller I, Spencer T, Tapsell S. Coastal flooding and
climate change. In: Health effects of climate change in the UK:
an expert review for comment. London: Department of Health;
2001, pp. 177-87.
9. Howard MJ, Brillman MD, Burkle FM. Infectious disease
emergencies in disasters. Emerg Med Clin North Am 1996; 14:
413-28.
10. Reacher M, McKenzie K, Lane C, Nichols T, Kedge I,
Iversen A, et al. Health impacts of flooding in Lewes: a
comparison of reported gastrointestinal and other illness and
mental health in flooded and non-flooded households. Commun
Dis Public Health 2004; 7: 39-46.
11. Du W, FitzGerald GJ, Clark M, Hou XY. Health impact of
floods. Prehosp Disaster Med 2010; 25: 265-72.
12. Few R, Ahern M, Matthies F, Kovats RS. Floods, health and
climate change: a strategic review. Tyndall Centre Working
Paper 63. Norwich: University of East Anglia; 2004.
13. Parker D, Thompson P. Floods in Africa: vulnerability, impacts
and mitigation. In: Parker D, ed. Floods. London: Routledge;
2000 pp. 188-203.
14. Wisner B, Blaikie P, Cannon T, Davis I. At risk: natural hazards,
people’s vulnerability and disasters. London: Routledge; 2004.
15. Kunii O, Nakamura S, Abdur R,Wakai S. The impact on health
and risk factors of the diarrhoea epidemics in the 1998
Bangladesh floods. Public Health 2002; 116: 68-74.
16. Bennet G. Bristol floods 1968: controlled survey of effects on
health of local community disaster. BMJ 1970; 3: 454-8.
17. Hajat S, Ebi L, Kovats S, Menne B, Edwards S, Haines A.
The human health consequences of flooding in Europe and
the implications for public health: a review. Extre Weathe Eve
Public Health Respo 2005: 185-96.
*Le Thi Thanh Ha,
Department of Epidemiology
Hanoi School of Public Health
138 Giang Vo street
Hanoi, Vietnam
Tel/Fax: 84-4-37365896
Email: ***@***.***
Recent Comments